Improving Outcomes for Diabetes Patients through Data Science
Data
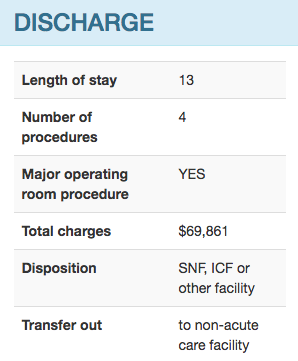
250,000 patients hospitalized with diabetes, 60+ Variables
Machine Learning Model
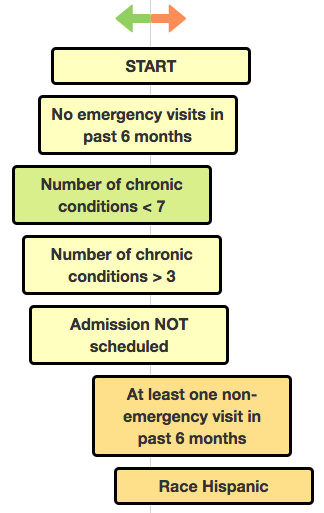
A rules-based decision tree to enable easy interpretation of risk factors
User Experience
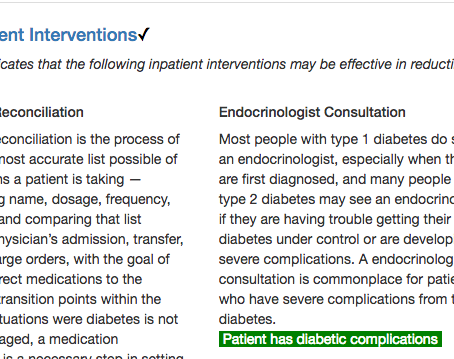
Timely insight for hospitals and medical professionals